Key Takeaways
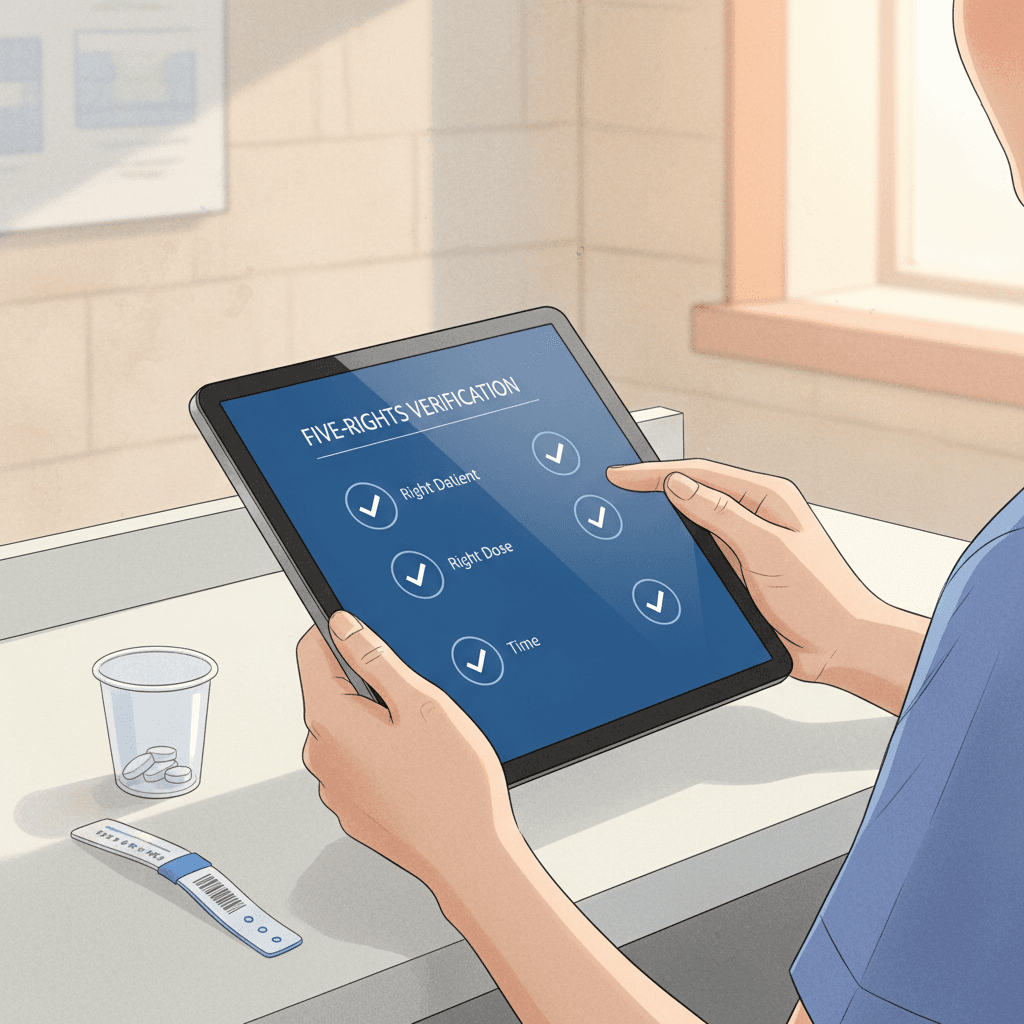
- The Five Rights of medication administration — right patient, right drug, right dose, right route, right time — remain the foundational safety framework in residential care, but implementation must be adapted to settings where staff know residents personally, pharmacy support may be limited, and unlicensed personnel may assist with medications.
- Identity verification in group homes and assisted living requires protocols beyond wristbands — photo verification, two-identifier checks at every administration, and systems that prevent assumption-based shortcuts even among familiar residents.
- Look-alike/sound-alike (LASA) drug errors account for up to 25% of all medication errors reported to safety organizations, and residential care settings face elevated risk because of the volume of oral solid medications administered during compressed med pass windows.
- The extended rights — right documentation, right reason, right response, and right to refuse — are not optional additions but essential complements that close safety gaps left by the original five, particularly in settings where residents have autonomy rights.
- Interruptions during medication administration are the single most studied and most persistent contributor to Five-Rights failures, with research showing a direct linear relationship between the number of interruptions and the probability of error.
- Electronic medication administration record (eMAR) systems reduce transcription errors, enforce verification steps, and create audit trails, but they cannot replace clinical judgment — technology is a verification layer, not a substitute for a trained clinician's assessment.
- Sustained medication safety requires a systems approach that combines protocol design, competency-based training, technology support, and a nonpunitive reporting culture — no single intervention is sufficient on its own.
Introduction
Medication errors are the single most common preventable adverse event in residential care. This is not a contested claim. It is a consistent finding across decades of patient safety research, regulatory data, and incident reporting systems in every jurisdiction that tracks adverse events in long-term care, group homes, and assisted living communities. The Institute for Safe Medication Practices, the World Health Organization, the National Coordinating Council for Medication Error Reporting and Prevention, and every major health authority that publishes residential care safety data arrive at the same conclusion: the medication system is where preventable harm most frequently originates.
The scale is difficult to absorb. In the United States alone, the Agency for Healthcare Research and Quality estimates that medication errors in long-term care facilities affect between 800,000 and 1.3 million residents annually. In England, the Care Quality Commission's state of care reports consistently identify medication management as one of the top three areas of regulatory concern. In Canada, provincial inspection data reveal that medication-related deficiencies appear in more than 40% of long-term care home inspections. In Australia, the Aged Care Quality and Safety Commission reports similar patterns. These are not fringe facilities. These are systemic findings across thousands of well-intentioned care organizations.
What makes medication errors particularly dangerous in residential care is their cascading nature. A single wrong-dose error — administering 10 milligrams of a blood pressure medication instead of 5 — does not resolve at the moment of discovery. It cascades through the next 72 hours of a resident's care. The resident's blood pressure drops. The evening nurse assesses the change but, without knowing about the dosing error, attributes it to the resident's existing cardiac condition and adjusts fluid intake. The night shift documents hypotension but does not escalate because the intervention appears to be working. By morning rounds, a physician reviewing the chart may order a medication change based on a clinical picture that was, in fact, caused by the original error. One mistake begets a chain of clinical decisions built on a false foundation.
The Five Rights of medication administration — right patient, right drug, right dose, right route, right time — exist to prevent that first error. They are the most widely taught, most frequently cited, and most fundamentally important safety framework in medication management. Every nurse learns them. Every medication administration policy references them. Every regulatory body expects them. And yet medication errors persist at rates that no other industry would tolerate for a process as standardized, as repetitive, and as well-understood as medication administration.
This guide examines why. It provides a detailed, practical implementation framework for applying the Five Rights in residential care settings — settings that differ meaningfully from hospitals in staffing models, pharmacy support, resident populations, and regulatory environments. It extends beyond the original five to address the additional rights that modern medication safety demands. It identifies the specific failure points where Five-Rights protocols break down in practice and offers evidence-based prevention strategies. And it addresses the role of technology — what it can solve, what it cannot, and what it must never be asked to replace.
The Five Rights Explained
The Five Rights of medication administration were first articulated in the 1960s as a teaching framework for nursing students. Over six decades, they have become the universal standard against which medication administration practice is measured. They are deceptively simple to state and extraordinarily difficult to execute with perfect consistency across thousands of administrations per month in a residential care setting. Each right deserves examination in the context where your staff actually practice — not a hospital ward with pharmacy verification systems, physician presence, and barcode scanners on every cart, but a 12-bed group home at 7:00 AM where one medication aide is administering oral medications to residents who are simultaneously eating breakfast, watching television, and asking about the day's activities.
Right Patient
The first right — confirming that the medication is being given to the correct resident — seems almost insultingly obvious. In a group home where a staff member has worked for three years and knows every resident by name, by voice, by the way they walk down the hallway, the idea of formally verifying identity before handing someone their morning pills can feel bureaucratic at best and absurd at worst. This sense of familiarity is precisely where right-patient errors originate.
The literature on wrong-patient errors in residential care consistently identifies the same root cause: assumption-based identification. A staff member "knows" which resident is which and skips the verification step. This works thousands of times. And then it fails once — when a new resident has moved into the room formerly occupied by someone else, when two residents with similar names are seated next to each other at the dining table, when a resident who normally stays in bed is up and walking and is encountered out of the context where the staff member expects to see them.
In hospitals, wrong-patient errors are mitigated by wristband scanning and two-identifier verification protocols. Residential care settings rarely use wristbands — residents live in these facilities, and a hospital-style wristband is inconsistent with the homelike environment that regulatory standards and families expect. The residential care equivalent requires a different approach: photograph-based identification in the medication administration record, a two-identifier protocol (name plus date of birth, or name plus room number, confirmed verbally or visually against the MAR), and a cultural expectation that verification is performed at every single administration, regardless of how well the staff member knows the resident.
The two-identifier check must be nonnegotiable. Not "when you're not sure." Not "for new residents." Every time. The reason is not that staff cannot recognize residents. The reason is that building the habit of checking every time eliminates the decision point — the moment where a busy, interrupted, fatigued staff member must decide whether this particular administration requires verification. That decision point is where errors enter. Eliminating it by making verification automatic — a reflex rather than a judgment call — is the only reliable prevention.
Right Drug
The second right requires confirming that the medication being administered is the medication that was prescribed. In residential care, right-drug errors take several forms: administering the wrong medication entirely, administering one resident's medication to another (which is simultaneously a right-patient and right-drug error), confusing two medications with similar names, and confusing two medications with similar physical appearance.
Look-alike/sound-alike (LASA) medications are a well-documented source of right-drug errors. Hydroxyzine and hydralazine. Metformin and metoprolol. Clonidine and clonazepam. Prednisone and prednisolone. The Institute for Safe Medication Practices maintains a list of confused drug names that exceeds 300 pairs. In residential care, where medications are frequently administered from pre-poured blister packs or multi-dose compliance packaging, the risk is compounded: the staff member administering the medication may not be the person who verified the pharmacy label against the prescriber's order. They are relying on a packaging and verification chain that occurred upstream.
Right-drug verification in residential care requires checking the medication name on the packaging against the medication administration record at the time of administration — not at the time of stocking, not at the time of receiving the pharmacy delivery, but at the moment the medication is about to be given to the resident. This is the point where the last human check occurs before the medication enters the resident's body. In settings using unit-dose or blister packaging, the drug name, strength, and physical description (color, shape, markings) should all be confirmed against the MAR entry. Any discrepancy — a pill that looks different from what was given yesterday, a label that seems slightly different, a medication that was not on the previous cycle's card — requires a hold-and-verify response: do not administer, contact the pharmacy or prescriber, and document the discrepancy.
Staff education on LASA risks specific to your facility's formulary is essential. Generic substitutions, manufacturer changes, and new admissions all introduce LASA exposure. A quarterly review of your facility's most commonly administered medications against the ISMP LASA list, with targeted education for any high-risk pairs, is a practical prevention measure that does not require technology to implement.
Right Dose
The third right — confirming that the correct dose is being administered — is more complex than it appears. In a hospital, pharmacist verification, computerized physician order entry, and automated dispensing systems create multiple checkpoints between the prescriber's intent and the patient's receipt. In residential care, these layers may be thinner or absent. A group home may receive pre-poured medications from a retail pharmacy with limited clinical pharmacist review. An assisted living community may have residents who self-administer from their own prescription bottles. A long-term care facility may have pharmacy services but still rely on nursing staff to calculate weight-based doses, split tablets, or reconstitute liquid formulations.
Right-dose errors in residential care include: administering the wrong strength (giving a 50 mg tablet when 25 mg was ordered, often because a strength change was ordered but the old supply was not removed), administering the wrong quantity (giving two tablets when one was ordered, or vice versa), failing to adjust for renal or hepatic function (particularly relevant for residents with fluctuating kidney function who require dose adjustments that may not be reflected in the pharmacy's blister pack), and mathematical errors in liquid dose calculations.
Dose verification requires comparing the dose on the MAR against the prescriber's current order and against the physical medication being administered. When the dose involves calculation — 7.5 mL of a 125 mg/5 mL suspension, for example — the calculation should be performed independently and documented. When dose adjustments are ordered (titration schedules, taper protocols, weight-based recalculations), the effective date and new dose must be reflected in the MAR before the next administration. One of the most common right-dose errors in residential care is a timing gap: the physician orders a dose change on Monday afternoon, the pharmacy updates the blister pack on Wednesday, and the resident receives the old dose on Tuesday because the MAR was not updated to reflect the change during the interim period.
Age-adjusted dosing adds another layer. Residential care populations are overwhelmingly geriatric, and geriatric pharmacology differs from adult pharmacology in clinically significant ways. Reduced renal clearance, altered volume of distribution, decreased hepatic metabolism, and increased sensitivity to central nervous system depressants all affect appropriate dosing. The right dose for a 70-year-old with a creatinine clearance of 60 mL/min is not the same as the right dose for a 35-year-old with normal renal function, even though the prescriber may have ordered the standard adult dose. Clinical staff administering medications in residential care need the pharmacological literacy to recognize when a dose appears inconsistent with the resident's clinical profile and to query the prescriber before administering.
Right Route
The fourth right — confirming that the medication is being administered by the correct route — is sometimes treated as self-evident. Most medications in residential care are oral. But "oral" itself encompasses multiple delivery methods: swallowed whole, chewed, dissolved under the tongue, dissolved in water, administered via enteral tube. And residential care settings also involve topical medications (creams, ointments, patches), ophthalmic and otic drops, inhalation medications, rectal suppositories, vaginal preparations, and — in some long-term care settings — subcutaneous injections (insulin, anticoagulants, some biologics).
Right-route errors in residential care most commonly involve: crushing a medication that should not be crushed (extended-release formulations, enteric-coated tablets), administering a sublingual medication orally (nitroglycerin placed on the tongue and swallowed instead of held under the tongue), applying a topical medication to the wrong site or failing to remove a previous patch before applying a new one (fentanyl patch errors are a recurring concern in long-term care), and administering an enteral tube medication without proper flushing technique or without confirming tube placement.
The crush-or-no-crush decision is particularly important in residential care because of the high prevalence of dysphagia in the geriatric population. A resident who develops swallowing difficulty may be switched to crushed medications, and staff must verify — not assume — which of that resident's medications can be safely crushed and which require a formulation change (liquid, dispersible tablet, alternative drug). Crushing an extended-release opioid, for example, releases the full dose at once instead of over 12 or 24 hours. This is not a minor inconvenience. It is a potentially lethal dosing error that has resulted in deaths documented in FDA safety communications and coroner reports.
In non-hospital residential settings, subcutaneous injection technique may be performed by staff with limited injection training. Insulin administration, in particular, requires verification of the injection site (rotation to prevent lipodystrophy), the needle length and gauge, the angle of injection, and the distinction between different insulin types that may look similar in pen or vial form. A right-route error in this context might involve injecting intramuscularly instead of subcutaneously because the needle length was inappropriate for the resident's body habitus, or failing to rotate sites because site rotation was not documented or tracked.
Right Time
The fifth right — administering the medication at the correct time — is the right that generates the most practical difficulty in residential care operations. A long-term care facility with 100 residents, each receiving an average of 8 to 12 medications, faces 800 to 1,200 medication administrations per day. These are distributed across scheduled times (0800, 1200, 1700, 2100 are common windows), PRN administrations (as needed, with clinical criteria that must be assessed before each dose), and time-critical medications that must be administered within a narrow window to maintain therapeutic effect.
Time-critical medications include: insulin (timed to meals), anticonvulsants (where a missed dose can lower the seizure threshold), antibiotics on strict interval schedules (every 6 hours means every 6 hours, not "four times a day whenever convenient"), antiparkinson medications (where even a 30-minute delay can cause significant symptom breakthrough), and immunosuppressants. The Centers for Medicare and Medicaid Services defines time-critical medications as those where an early or late administration of more than 30 minutes could cause harm or have a significant negative clinical impact. Non-time-critical medications have a broader administration window, typically within one to two hours of the scheduled time.
Right-time failures in residential care often stem from operational constraints rather than knowledge gaps. The med pass itself takes time. A nurse administering medications to 30 residents on a morning pass may need 90 minutes or more. Residents who are in the shower, at therapy, sleeping, or in the dining room must be found and returned to, which adds time and interrupts the sequence. PRN medications requested during a scheduled pass create competing priorities. And staffing shortfalls — a nurse calling in sick, an aide pulled to another unit — compress the available time further.
The distinction between scheduled and PRN medications is a right-time issue that deserves separate attention. PRN medications require clinical assessment before each administration: Does the resident meet the criteria for this medication? When was the last dose? Has the minimum interval elapsed? Is there a maximum daily dose that has been reached? These questions are not time-of-day questions but temporal-sequence questions, and they require access to the resident's recent administration history. A PRN acetaminophen ordered "every 4 hours as needed for pain, maximum 3 grams per day" requires the administering staff to know when the last dose was given, how many doses have been given today, and whether the resident's total daily acetaminophen intake (including combination products) has reached the ceiling. In a paper-based MAR system, this information may be scattered across multiple pages. In an eMAR system, it can be calculated and displayed automatically — one of the clearest advantages of electronic medication records for right-time verification.
Beyond the Five: The Extended Rights
The original Five Rights, while foundational, were designed for a clinical environment where medication administration was a task performed by registered nurses in acute care hospitals. Residential care has evolved into a setting where medication management intersects with resident autonomy, informed consent, regulatory documentation requirements, and outcome monitoring in ways that the original five do not fully address. Four additional rights — sometimes called the extended rights — have been adopted by medication safety organizations and regulatory bodies to close these gaps.
Right Documentation
The sixth right: document every administration. This includes what was given, the dose, the route, the time, the identity of the person who administered it, and any relevant observations (resident's response, refusal, reason for holding a dose). Right documentation is not merely a record-keeping requirement. It is a safety mechanism. The next staff member who administers a medication to this resident will rely on the documentation trail to make dosing decisions, assess intervals, and evaluate therapeutic response. A PRN pain medication administered at 2:00 PM but not documented until the nurse remembers at 6:00 PM creates a four-hour window during which another staff member could administer a second dose without knowing the first was given.
In residential care, right documentation faces a structural challenge: the person administering the medication and the person documenting the administration are not always the same person, and they are not always documenting in real time. In group homes where a single staff member is administering, supervising, and documenting, the temptation to batch-document — administer to all residents first, then document for all residents afterward — is strong. This practice is explicitly prohibited by most regulatory standards because it severs the temporal link between administration and documentation, introduces memory-based errors, and makes it impossible to determine whether a dose was actually given or merely intended.
Point-of-care documentation — documenting at the time and place of administration — is the standard. Whether that documentation occurs on a paper MAR at the medication cart or on a mobile device running an eMAR application, the entry must be made at the time the medication is given. Not after the med pass. Not at the end of the shift. At the time.
Right Reason
The seventh right: the clinician administering the medication should understand why the resident is receiving it. This is not about pharmacological expertise — it is about clinical context. A medication aide administering metoprolol should know that it is a blood pressure medication and that the resident's heart rate should be checked before administration. A nurse administering lorazepam should know that it is prescribed for the resident's anxiety and should assess whether the resident is currently exhibiting symptoms that warrant a dose (if it is PRN) or whether there are contraindications present (excessive sedation, respiratory depression) that should prompt holding the dose and contacting the prescriber.
Right reason serves as a secondary safety check. If a staff member does not know why a medication is prescribed and notices something unusual — a new medication on the MAR, a change in dose, a medication that seems inconsistent with the resident's known conditions — the right-reason principle gives them standing to question the order. In residential care, where the prescriber is rarely on-site and orders are received by phone, fax, or electronic transmission, the administering clinician is often the last clinical checkpoint before the medication reaches the resident. A culture that values right-reason thinking empowers that clinician to say, "This does not seem right — I need to verify before I give it."
Right Response
The eighth right: after administering a medication, the clinician should monitor for the expected therapeutic response and for adverse effects. Did the pain medication reduce the resident's pain? Did the antihypertensive lower blood pressure to the target range? Did the antibiotic produce any allergic reaction? Right response closes the feedback loop. A medication that is consistently administered without producing the desired effect is a medication that needs to be re-evaluated — not continued indefinitely because it is on the MAR.
In residential care, right-response monitoring is often underdeveloped. The sheer volume of medications administered can make it impractical to formally assess the outcome of every dose. But for high-risk medications — opioids, anticoagulants, insulin, antipsychotics, antiepileptics — post-administration monitoring is a safety-critical practice. A resident receiving a new opioid should have pain reassessment within an hour. A resident whose insulin dose was recently adjusted should have blood glucose monitoring on a defined schedule. A resident started on an antipsychotic should be assessed for extrapyramidal symptoms, sedation, and metabolic effects on a recurring basis.
Right to Refuse
The ninth right: a competent resident has the right to refuse any medication. This right sits at the intersection of medication safety and resident autonomy, and it is particularly significant in residential care where the line between persuasion and coercion can become blurred. A resident who refuses their morning blood pressure medication is exercising a legal right. The staff member's obligation is to explain (within their scope of practice) why the medication is important, document the refusal and the explanation given, notify the prescriber, and document the notification. The staff member does not have the authority to insist, to hide the medication in food without consent, or to record the medication as given when it was refused.
Covert administration — placing medication in food or drink without the resident's knowledge — is a practice that requires explicit legal authorization in most jurisdictions (court order, power of attorney consent, or specific regulatory provision) and a documented clinical justification. It is never appropriate as a convenience measure because a resident is "difficult" about medications. Where covert administration is legally authorized, it must be documented in the care plan with the legal basis, the specific medications involved, and the method of covert administration.
Refused medications that are not documented create two safety problems: the resident does not receive the therapeutic benefit of the medication, and the medical record falsely implies that they did. Over time, undocumented refusals can mask a pattern — a resident who consistently refuses a particular medication may be experiencing side effects they cannot articulate, may have lost the ability to swallow pills and is refusing out of fear of choking, or may be exercising a preference about their own care that should be incorporated into the care plan.
Verification Protocols for Residential Settings
Implementing the Five Rights requires verification protocols that are specific to the care setting. A protocol designed for a hospital pharmacy dispensing system will not function in a 12-bed group home without a pharmacist on-site. A protocol designed for a group home will not scale to a 120-bed long-term care facility with multiple units and shift changes. The verification approach must match the operational reality.
Group Homes Without Pharmacy Systems
Group homes — particularly small residential care settings with 4 to 16 beds — often receive medications from retail pharmacies in standard prescription vials or bubble packs. There may be no pharmacist review of the medication administration record. There may be no unit-dose packaging. The staff administering medications may be medication aides or unlicensed assistive personnel operating under delegated authority, not registered nurses.
In this setting, verification relies heavily on the medication administration record as the single controlling document. The MAR must be reconciled against the original prescriber orders at the time of setup and at every pharmacy delivery. Each administration requires a four-point check: resident identity (two identifiers), medication name and strength on the label matched to the MAR entry, correct number of units or measured volume, and scheduled time confirmed. The staff member must initial the MAR at the time of administration, and any discrepancy — a pill that looks unfamiliar, a count that does not match, a time that seems wrong — must trigger a stop-and-verify response.
The absence of electronic verification in many group home settings makes the paper MAR the critical safety artifact. MARs must be legible, current, free of unauthorized corrections (single-line strikethrough with initials, never white-out or erasure), and reviewed by a licensed nurse on a defined schedule (weekly is common; monthly is minimum). Transcription errors at MAR setup are a known failure point: the person transferring the prescriber's order to the MAR may copy the drug name incorrectly, misread the dose, or misinterpret the frequency. A pharmacist or nurse verification step at the point of MAR creation is a cost-effective safety measure.
Long-Term Care With 100+ Residents
Larger long-term care facilities face a different verification challenge: scale. With 100 or more residents, each receiving 8 to 12 medications, the medication system processes 1,000 or more administrations daily. The med pass — the window during which scheduled medications are administered — is a high-volume, high-pressure period where the conditions for error are maximized: time pressure, interruptions, multiple residents, similar medications, concurrent demands.
Verification at this scale requires system-level controls in addition to individual clinician practice. Automated dispensing or pre-verification by a consultant pharmacist ensures that the medications arriving on the unit have been checked for appropriateness, interactions, and accuracy before the nurse begins the pass. The nurse's role is then to verify at the point of administration — confirming the five rights against the MAR — rather than to perform the entire verification chain alone.
Medication cart organization is a verification enabler. Carts organized by resident, with medications in the same sequence as the MAR, reduce the time and cognitive effort required for each verification. Carts that mix residents, require searching for the correct drawer, or contain medications for residents on different units introduce opportunities for selection error.
Assisted Living With Self-Administration
Assisted living communities occupy a regulatory middle ground. Residents may self-administer medications (retaining their own prescriptions and managing their own dosing schedules) or may receive assistance from staff, depending on the regulatory framework of the jurisdiction and the resident's functional capacity. Self-administration means the Five Rights are the resident's responsibility — but the facility retains an obligation to monitor, to intervene when self-administration is no longer safe, and to document the resident's self-administration capacity in the care plan.
When staff assist with medications in assisted living — cueing, reminding, opening containers, reading labels — the Five-Rights verification is adapted to the level of assistance. A staff member who hands a resident their prescription bottle and reminds them to take their morning dose is performing a different function than a nurse who selects the medication, verifies the dose, and places it in the resident's hand. The verification obligations differ accordingly, but the principle is the same: at whatever level of assistance is being provided, the person providing it must confirm, to the extent of their role, that the right medication is going to the right person.
Verification Checklist
At the point of every medication administration, regardless of setting, the administering individual should confirm:
- Resident identity: Verified using two identifiers (name plus date of birth, name plus photograph, name plus room number). Verbal confirmation from the resident when cognitively able.
- Medication match: Drug name and strength on the label or package match the MAR entry exactly. Physical appearance of the medication (color, shape, markings) is consistent with prior administrations.
- Dose accuracy: Number of units, volume of liquid, or other measurement matches the ordered dose. Calculations have been performed and verified.
- Route confirmation: The ordered route (oral, topical, sublingual, subcutaneous, etc.) matches the formulation being administered. Crush/no-crush status confirmed for oral medications.
- Time verification: The current time falls within the acceptable administration window for this medication. For PRN medications: last dose time and daily maximum confirmed. For time-critical medications: administration within 30 minutes of scheduled time.
- Allergy check: Resident's documented allergies have been reviewed. No known allergy to the medication being administered.
- Clinical assessment: For medications requiring pre-administration assessment (blood pressure before antihypertensives, heart rate before beta-blockers, blood glucose before insulin), the assessment has been performed and the result supports administration.
Common Failure Points
Understanding where Five-Rights protocols break down is as important as understanding the protocols themselves. Medication errors do not occur randomly. They cluster around specific operational conditions, workflow patterns, and system design failures that are predictable and, therefore, preventable.
Interruptions During Med Pass
The evidence on interruptions and medication errors is extensive, consistent, and unambiguous. Every study that has examined the relationship between interruptions during medication administration and error rates has found the same thing: more interruptions produce more errors. The relationship is linear and dose-dependent. A nurse who is interrupted once during a medication pass is measurably more likely to make an error than a nurse who is not interrupted. A nurse who is interrupted six or more times during a pass has a dramatically elevated error probability.
In residential care, interruptions during med pass are endemic. Residents ask questions. Family members approach the nurse. Call lights sound. CNAs need direction. Phones ring. A resident in the dining room needs assistance. A delivery arrives. An incident occurs on another unit. Each interruption forces the nurse to break concentration, attend to the interrupting stimulus, and then return to the medication task — often without returning to the exact point in the verification process where they left off. The most dangerous scenario is an interruption between selecting the medication and administering it, because the nurse may resume with a different medication or a different resident without re-verifying.
Prevention strategies include: designated "do not disturb" protocols during med pass (signage, verbal announcements, alternative points of contact for non-urgent issues), medication administration vests or sashes that signal unavailability, restructured workflows that separate medication administration from other nursing tasks, and organizational policies that treat interruptions during med pass as safety events to be tracked and reduced.
Delegation to Unlicensed Staff
In many jurisdictions, medication administration in residential care may be delegated to unlicensed assistive personnel — medication aides, medication technicians, or trained care aides — who operate under the delegation and supervision of a licensed nurse. The regulatory frameworks for this delegation vary dramatically. In some Canadian provinces, Loi 90 (Quebec's professional code reform) expanded the scope of unlicensed workers to include medication administration under specific conditions. In some US states, medication aides can administer routine oral medications after completing a state-approved training program. In others, only licensed nurses may administer any medication.
The Five-Rights framework applies regardless of the licensure status of the person administering, but the risk profile differs. Unlicensed staff may have less pharmacological knowledge, less ability to recognize clinical situations that warrant holding a dose, less experience with calculating doses, and less training in assessment techniques required before certain medications. The delegation framework must include: clear identification of which medications can be administered by unlicensed staff and which are restricted to licensed personnel (insulin, narcotics, and PRN medications with complex criteria are commonly restricted), competency assessment before and periodically after delegation, accessible supervision (the delegating nurse must be available for questions and consultation), and defined escalation pathways for any situation where the unlicensed person is uncertain.
Narcotic Count Discrepancies
Controlled substance management in residential care is a Five-Rights issue that carries both clinical and legal dimensions. Narcotics must be counted at every shift change, and discrepancies must be investigated immediately. But the count itself is only one element. Right-drug and right-dose verification for controlled substances must be performed with particular rigor because the consequences of error are severe — both for the resident (overdose, respiratory depression) and for the staff member (regulatory investigation, criminal liability if diversion is suspected).
Common narcotic management failures include: failure to perform two-person verification at the time of administration, failure to count at shift change (or performing the count pro forma without actually verifying the physical inventory against the log), transcription errors in the narcotic log that create apparent discrepancies requiring time-consuming investigation, and failure to waste partial doses with a witness. Prevention requires a zero-tolerance discrepancy resolution policy: any count that does not match is investigated before the oncoming shift assumes responsibility, and the investigation is documented regardless of whether the discrepancy is resolved.
PRN Without Clear Criteria
PRN (as needed) medications present a Five-Rights challenge because the "right time" is not a clock time but a clinical determination. The prescriber's order defines the criteria: "lorazepam 0.5 mg PO every 6 hours PRN for acute anxiety with documented behavioral symptoms." The administering clinician must assess whether the criteria are met, whether the interval has elapsed, and whether the daily maximum has been reached. When the criteria are vague — "PRN for agitation" without defined behavioral indicators — the right-time determination becomes subjective, and different staff members will apply different thresholds. This leads to both overuse (administering when the criteria are marginally met) and underuse (withholding because the staff member is unsure whether the criteria are met).
Facilities should work with prescribers to ensure that every PRN order includes: specific clinical criteria for administration, a defined interval between doses, a maximum daily dose, and required monitoring after administration. Orders that lack these elements should be clarified before the medication is administered. The MAR should capture not only that a PRN medication was administered but the clinical assessment that justified the administration — what the resident was exhibiting, what nonpharmacological interventions were attempted first (where applicable), and the planned follow-up assessment.
Refused Medications Not Documented
As discussed under the right to refuse, undocumented refusals are a safety and compliance failure. Staff may fail to document refusals for several reasons: they do not consider a refusal a clinical event requiring documentation, they are embarrassed that they could not persuade the resident, they intend to return later and try again (and then forget), or they are unsure how to document a refusal in their MAR system. The result is a record that shows the medication as neither given nor refused — a gap that raises questions in any review.
The documentation standard for a refused medication is: the time of the refusal, the reason for refusal if the resident states one, the education or explanation provided, the notification of the prescriber (for time-critical or clinically significant medications), and any follow-up actions. This documentation serves multiple purposes: it protects the staff member and the facility from allegations that the medication was not offered, it creates a pattern record that may inform care plan changes, and it alerts the prescriber to the need for alternative approaches or formulations.
Medication Errors During Transitions
Transitions — admissions, discharges, hospital returns, transfers between units — are high-risk periods for Five-Rights failures. A resident returning from a hospital stay may have a completely different medication regimen: some medications discontinued, others started, doses changed, routes altered. The medication reconciliation process — comparing the pre-hospital medication list with the discharge medication list and producing a current, accurate list of what the resident should now be receiving — is a critical safety step that is frequently performed under time pressure and without all necessary information.
The most dangerous transition error is a duplication: a medication that was changed in the hospital but not discontinued in the facility's system, resulting in the resident receiving both the old and new medications. The second most dangerous is an omission: a medication started in the hospital that does not get transferred to the facility's MAR, resulting in a therapeutic gap. Both errors are preventable with a structured medication reconciliation protocol performed by a licensed clinician before the first post-transition medication administration.
Technology Support for Five-Rights
Technology does not eliminate medication errors. This statement must precede any discussion of technology's role in medication safety because the history of healthcare technology adoption is littered with implementations that introduced new error types while reducing old ones. With that caveat firmly in place, the evidence does support that specific technologies, properly implemented, meaningfully reduce the frequency of Five-Rights failures.
Electronic Medication Administration Records (eMAR)
eMAR systems replace paper MARs with electronic records that are updated in real time at the point of care. The safety advantages are substantial. An eMAR eliminates transcription errors because the medication order flows from the prescriber (or pharmacy) to the MAR electronically, without a human transcription step. It enforces right-time verification by displaying the administration window and alerting the clinician when a medication is being administered outside the acceptable window. It calculates PRN intervals and daily maximums automatically, preventing interval and ceiling violations. It creates a time-stamped, user-identified audit trail for every administration, hold, refusal, and waste.
An eMAR also supports right-patient verification through resident photograph display, reducing identity errors in settings where wristbands are not used. Some eMAR systems integrate barcode verification: the clinician scans the resident's identifier (a barcode on the MAR, on a photograph card, or on a discreet wristband) and the medication package barcode; the system confirms or rejects the match before allowing documentation of the administration.
Drug Interaction Alerts
Clinical decision support integrated into eMAR or electronic health record systems can alert the administering clinician to drug-drug interactions, drug-allergy contraindications, therapeutic duplications, and dose range violations. These alerts serve as a real-time second check on the prescriber's order and the pharmacist's review. In residential care, where consultant pharmacist reviews may occur monthly rather than per-order, real-time alerts provide a safety net that catches errors that passed through earlier verification stages.
Alert fatigue — the phenomenon where clinicians become desensitized to alerts because of their volume and frequency — is a legitimate concern. Systems that generate alerts for clinically insignificant interactions (mild interactions, interactions already accounted for by the prescriber) train clinicians to override alerts reflexively, which defeats the purpose. Effective alert systems are tiered: high-severity alerts (potentially lethal interactions, absolute contraindications) are hard stops that require clinical override documentation; moderate-severity alerts are informational but documented; low-severity alerts are suppressed or batched for pharmacist review.
Automated Narcotic Counts
Automated dispensing cabinets and electronic narcotic logs reduce the clerical burden of controlled substance tracking and improve the accuracy of count reconciliation. When a nurse removes a controlled substance from an automated cabinet, the system records the identity of the nurse, the medication, the dose, the resident, and the time. Count discrepancies are flagged immediately, and the system generates audit trails that support both clinical safety and regulatory compliance. In facilities where automated dispensing is not feasible, electronic narcotic logging — even a simple application that replaces the paper narcotic log — reduces mathematical errors in count reconciliation and provides a more reliable audit trail.
What Harmony's Medication Module Provides
Harmony's medication management module is designed specifically for residential care settings — not adapted from a hospital system, but built for the workflows, staffing models, and regulatory requirements that group homes, long-term care facilities, and assisted living communities actually operate under. The module includes eMAR functionality with resident photograph display, barcode verification capability, real-time drug interaction and allergy alerts, automated PRN interval and ceiling tracking, narcotic count integration, and medication reconciliation tools for transitions of care. Configurable alert thresholds allow facilities to tune the clinical decision support to their formulary and population, reducing alert fatigue while maintaining protection for high-severity events.
What Technology Cannot Replace
No technology replaces the clinical judgment of the person standing in front of the resident. An eMAR can confirm that the medication matches the order. It cannot assess whether the resident's current clinical condition warrants holding the dose. A barcode scanner can confirm that the pill is the right pill. It cannot notice that the resident is more lethargic than usual, that their breathing pattern has changed, or that they are holding their jaw in a way that suggests they will have difficulty swallowing. An interaction alert can flag a potential drug-drug interaction. It cannot weigh the clinical context — the resident's history, the severity of the condition being treated, the alternatives available — that determines whether the interaction risk is acceptable.
Technology is a verification layer. It adds checkpoints to the Five-Rights process. It reduces the types of errors that arise from transcription, calculation, memory, and information access. It does not reduce the types of errors that arise from clinical inattention, knowledge deficits, or impaired judgment. The combination of technology and competent clinical practice produces medication safety. Neither alone is sufficient.
Case Scenario: Greenfield Residential
Greenfield Residential operates a 64-bed long-term care facility in a mid-sized metropolitan area. The facility serves a mixed population: approximately 40 residents with moderate to severe cognitive impairment, 15 with complex medical needs requiring skilled nursing, and 9 in a transitional care program. The nursing staff includes 4 registered nurses, 8 licensed practical nurses, and 12 certified nursing assistants across three shifts. Medications are supplied by a contract pharmacy that delivers weekly in blister-pack format with a monthly consultant pharmacist review.
In the twelve months before implementing a structured Five-Rights protocol supported by an eMAR system, Greenfield tracked an average of 4.2 medication errors per month through its incident reporting system. The medication error rate — calculated as errors per 1,000 administrations — was 2.1, which was consistent with industry benchmarks but unacceptable to the facility's clinical leadership. The errors included wrong-time administrations (38%), wrong-dose errors (22%), missed doses (19%), wrong-patient errors (11%), and wrong-route errors (10%).
The clinical director's analysis revealed several contributing factors. Paper MARs were being transcribed from pharmacy labels by the unit nurses, introducing transcription errors at the point of MAR setup. PRN medication intervals were being tracked manually, and two wrong-interval errors had resulted in doses being given before the minimum interval had elapsed. Narcotic counts were reconciling successfully but consuming 25 minutes per shift change — time the clinical director wanted to redirect to clinical care. And med pass interruptions had never been measured but were estimated by nursing staff to average 8 to 12 per pass.
Greenfield implemented three concurrent changes. First, the facility deployed Harmony's eMAR module, replacing paper MARs with electronic records that received medication orders directly from the pharmacy's dispensing system, eliminating transcription. Resident photographs were added to every electronic MAR record. PRN tracking was automated, with alerts preventing administration before the minimum interval or beyond the daily maximum. Second, the facility implemented a "Sacred Med Pass" policy: during scheduled medication passes, the administering nurse wore a medication safety vest, and all non-urgent communications were directed to a designated charge nurse or CNA. Interruption counts were tracked for the first 90 days. Third, the facility implemented a quarterly Five-Rights competency assessment for all staff with medication administration responsibilities, using simulation scenarios that tested each right under realistic conditions, including interruption simulation.
Over the following twelve months, Greenfield's monthly medication error rate dropped from 4.2 to 0.3 — a 93% reduction. Wrong-time errors, which had been the largest category, decreased from 1.6 per month to 0.1, driven almost entirely by the eMAR's automated time window enforcement and PRN interval tracking. Wrong-dose errors decreased from 0.9 per month to 0.08, driven by the elimination of transcription errors and the dose range alerts. Interruptions during med pass decreased by 67% in the first 90 days and remained at the reduced level thereafter. Narcotic count reconciliation time decreased from 25 minutes to 6 minutes per shift change with the electronic narcotic log.
The clinical director attributed the sustained improvement to the combination of technology and culture change. "The eMAR caught the errors that come from information gaps — wrong times, wrong intervals, wrong transcriptions," she reported. "But the Sacred Med Pass policy changed how the building functions during med pass. Staff stopped treating the nurse as the person to ask about everything. They started protecting the med pass the way an operating room protects the surgical count. That cultural shift was as important as the technology."
Training and Competency
A Five-Rights protocol is only as reliable as the competency of the staff executing it. Competency is not knowledge alone — it is the demonstrated ability to perform the correct verification steps under realistic conditions, including the time pressure, interruptions, and competing demands that characterize actual medication administration in residential care. A staff member who can recite the Five Rights on a written exam but skips right-patient verification when they are behind schedule during the morning med pass does not have functional competency.
Initial Training
New hire medication training should be structured, competency-gated, and practical. Classroom instruction on the Five Rights, medication safety principles, and the facility's specific medication policies establishes the knowledge foundation. But knowledge must be translated into skill through supervised practice: the new hire administers medications under direct observation by a preceptor for a defined number of administrations (not a defined number of days — competency is measured by performance, not by calendar), and the preceptor verifies that all Five Rights are being performed at every administration before signing off.
The training should include facility-specific content: the types of medications most commonly administered, the LASA risks present in the facility's formulary, the specific verification steps required by the eMAR or paper MAR system, the escalation pathway for questions or discrepancies, and the documentation requirements for refusals, holds, and PRN administrations. Generic medication safety training that covers the Five Rights in abstract without connecting them to the specific workflows and systems the staff member will actually use produces knowledge without skill.
Annual Competency Assessments
Annual competency reassessment ensures that Five-Rights practice has not degraded over time. Competency should be assessed through direct observation of actual medication administrations (not simulated ones) by a clinical supervisor, supplemented by simulation scenarios that test specific risk situations: a medication that looks different from the usual supply, a resident who is encountered out of their usual location, a PRN request during a scheduled pass, a controlled substance administration requiring two-person verification, a new order that appears inconsistent with the resident's diagnosis.
The assessment should use a structured rubric that maps to each of the Five Rights (and extended rights) with pass/fail criteria. A staff member who consistently verifies drug, dose, route, and time but skips resident identification has a competency gap that requires targeted remediation — not blanket retraining. The assessment should also include a knowledge component: questions about the facility's LASA list, the crush/no-crush policy, the PRN documentation requirements, and the escalation pathway for discrepancies.
Simulation Exercises
Simulation-based training offers the ability to expose staff to high-risk scenarios without risking resident harm. Effective simulation exercises for Five-Rights competency include:
- Interruption simulation: The staff member is administering medications to a standardized "resident" when a colleague approaches with a non-urgent question. The assessment measures whether the staff member completes the current verification step before responding, or abandons the verification mid-process.
- LASA confusion: Two medications with similar names or appearances are placed on the medication cart. The scenario tests whether the staff member catches the discrepancy during right-drug verification.
- Wrong-patient setup: Medications for Resident A are placed in Resident B's drawer. The scenario tests whether the staff member's identity verification catches the mismatch before administration.
- Dose change lag: A dose change has been ordered but the pharmacy supply has not yet been updated. The scenario tests whether the staff member identifies the discrepancy between the MAR (showing the new dose) and the physical medication (showing the old dose).
- PRN threshold: A resident requests pain medication. The scenario provides clinical information that places the request in a gray area relative to the PRN criteria. The assessment measures whether the staff member assesses against the criteria, documents the assessment, and makes a defensible clinical decision.
Sustaining Competency Culture
Training events — initial orientation, annual assessments, simulation exercises — are necessary but not sufficient. Sustained Five-Rights competency requires a cultural environment where medication safety is treated as a core professional value rather than a compliance checkbox. This culture has several characteristics: medication errors are reported without fear of punitive consequences (a just culture), reported errors are investigated for system causes rather than individual blame, near-misses are valued as safety intelligence, Five-Rights compliance is recognized and reinforced (not just Five-Rights failures that are corrected), and frontline staff participate in designing and improving the medication safety system rather than simply being subject to it.
Leadership visibility matters. When the director of nursing periodically observes a med pass and provides specific positive feedback on Five-Rights practice, it signals that medication safety is a leadership priority, not just a policy requirement. When medication safety data — error rates, near-miss reports, interruption counts — are shared with staff transparently, it creates a shared understanding of the problem and the progress. When staff suggestions for improving the medication system are implemented and acknowledged, it builds the engagement that sustains compliance long after the training event has ended.
Conclusion
The Five Rights of medication administration are not a checklist to be completed and filed. They are a cognitive framework that must be executed — fully, correctly, and without exception — at every single medication administration, every day, across every shift, in every residential care setting. In a facility administering 1,000 medications per day, that is 1,000 opportunities to prevent harm and 1,000 opportunities for harm to occur. The margin between a medication error rate of 2.0 per 1,000 administrations and 0.3 per 1,000 administrations is not the difference between negligent and excellent care. It is the difference between a system that relies on individual vigilance alone and a system that supports individual vigilance with verification protocols, technology safeguards, competency assurance, and a culture that treats every deviation as a signal rather than a statistic.
The extended rights — right documentation, right reason, right response, right to refuse — address the dimensions of medication safety that the original five were never designed to cover. They are not optional enhancements. They are essential complements in a residential care environment where residents have autonomy rights, where documentation is the legal record of care, and where post-administration monitoring closes the feedback loop between medication delivery and therapeutic outcome.
Technology — eMAR systems, barcode verification, drug interaction alerts, automated narcotic tracking — provides the verification infrastructure that makes consistent Five-Rights practice achievable at scale. It eliminates entire categories of errors that arise from transcription, calculation, memory, and information access limitations. But technology is a layer, not a replacement. The clinician at the bedside, at the medication cart, at the dining room table where a resident takes their morning pills — that clinician's competence, attention, and commitment to verification is where medication safety ultimately lives.
Every residential care organization has the ability to implement the Five-Rights framework described in this guide. The protocols are not complex. The technology is available. The training methods are established. The evidence base is clear. What is required is the organizational decision to treat medication safety not as one priority among many but as the nonnegotiable foundation on which every other aspect of care quality depends. Because it is. A resident whose medications are administered safely — right patient, right drug, right dose, right route, right time, right documentation, right reason, right response, right to refuse — is a resident whose care team has met the most fundamental obligation of clinical practice: first, do no harm.
Frequently Asked Questions
What is the difference between the Five Rights and the extended rights of medication administration?
The original Five Rights — right patient, right drug, right dose, right route, right time — focus on the physical act of administering the correct medication to the correct person. They were developed in the 1960s as a teaching framework for nursing students in acute care settings. The extended rights — right documentation, right reason, right response, and right to refuse — address the broader clinical context of medication administration: recording what was done, understanding why it was done, monitoring the outcome, and respecting the resident's autonomy. In residential care, where residents live in the facility long-term and where documentation, monitoring, and autonomy are central to quality of life and regulatory compliance, the extended rights are essential complements to the original five. Together, the nine rights provide a comprehensive framework for medication safety.
How often should Five-Rights competency be assessed for medication administration staff?
Best practice calls for competency assessment at three points: during initial orientation before independent medication administration is permitted, annually as part of the organization's ongoing competency program, and whenever a medication error or near-miss suggests a competency gap. The assessment should include direct observation of actual medication administrations using a structured rubric that evaluates each right individually, supplemented by simulation scenarios that test performance under realistic conditions such as interruptions, LASA confusion, and PRN decision-making. Staff who do not meet the competency standard require targeted remediation and reassessment before resuming independent medication administration.
Can unlicensed staff administer medications in residential care settings?
The answer depends entirely on the jurisdiction. In many US states, certified medication aides may administer routine oral and topical medications in long-term care and assisted living after completing a state-approved training program. In Canada, the scope of medication administration by unlicensed workers varies by province, with Quebec's Loi 90 being a notable framework. In the United Kingdom, care workers in residential settings may administer medications under specific conditions. In all jurisdictions that permit delegation, the Five-Rights framework applies fully to unlicensed staff, and additional safeguards are typically required: supervision by a licensed nurse, restriction from administering high-risk medications (controlled substances, injectables, PRN medications with complex criteria), and documented competency assessment. Facilities should consult their jurisdiction's specific regulatory framework before establishing delegation practices.
What is the most effective way to reduce interruptions during medication administration?
The evidence supports a multi-layered approach. Visual cues — medication safety vests, tabards, or sashes worn by the administering nurse during med pass — reduce interruptions by 40 to 50% in studies that have measured the effect. Organizational policies that designate an alternative contact (a charge nurse, a CNA lead, a unit coordinator) for all non-urgent matters during med pass redirect interruptions away from the administering nurse. Physical environment modifications — medication preparation areas separated from high-traffic zones, closed medication rooms where available — reduce ambient interruptions. And cultural reinforcement — staff education on the interruption-error relationship, leadership modeling of non-interruption behavior, and tracking of interruption rates as a safety metric — sustain the behavioral changes over time. No single intervention is sufficient; the combination produces the most reliable reduction.
Does an eMAR system eliminate the need for manual Five-Rights verification?
No. An eMAR system automates several verification steps — it eliminates transcription errors, enforces administration time windows, calculates PRN intervals and daily maximums, displays resident photographs for identity verification, and generates alerts for drug interactions and allergy contraindications. These are significant safety improvements. But the eMAR cannot perform the clinical assessments that several rights require: checking blood pressure before administering an antihypertensive, assessing swallowing ability before giving an oral medication, evaluating whether a resident's current symptoms meet the criteria for a PRN dose, or recognizing that a resident is more sedated than usual and that an opioid dose should be held pending assessment. The eMAR is a verification layer that supports and strengthens the Five-Rights process. The clinical judgment of the administering staff member remains the primary safety mechanism and cannot be automated.